
Risk factors and survival of EBV-infected aplastic anemia patients after haploid allogeneic hematopoietic stem cell transplantation
-
摘要:
目的 分析再生障碍性贫血(AA)患者进行单倍体异基因造血干细胞移植(Haplo-HSCT)后EB病毒(EBV)感染危险因素及患者生存情况。 方法 回顾性分析2019年1月1日—2022年10月31日某院血液科78例进行Haplo-HSCT的AA患者临床资料,观察EBV血症、临床诊断的EBV相关性疾病(EBV病)及淋巴细胞增殖性疾病(PTLD)发生情况及出现时间,并分析其危险因素及生存情况。 结果 78例患者中男性38例,女性40例,中位年龄33(9~56)岁,其中53例患者发生EBV再激活,总发生率67.9%,发生EBV再激活的中位时间为移植后33(13, 416)d。EBV再激活患者中,单纯EBV血症49例(62.8%),可能的EBV疾病2例(2.6%),已经证实的EBV疾病(PTLD)2例(2.6%)。单因素提示,移植时患者年龄<40岁、脐血辅助回输、移植后发生急性移植物抗宿主病(aGVHD)、合并巨细胞病毒(CMV)感染是AA患者进行Haplo-HSCT后发生EBV再激活的独立危险因素,多因素分析提示合并CMV感染是AA患者进行Haplo-HSCT后发生EBV再激活的独立危险因素(P=0.048)。干细胞回输前使用利妥昔单抗干预是EBV再激活时间长短的影响因素(P<0.05)。单纯EBV血症病死率为8.2%,EBV病病死率为50.0%,PTLD病死率为100%。EBV再激活患者2年总生存率为85.3%,EBV未激活患者2年生存率为90.7%,差异无统计学意义(P=0.897),但应用利妥昔单抗治疗的患者其2年生存率低于未使用的患者,差异有统计学意义(P=0.046)。 结论 EBV再激活是AA患者进行Haplo-HSCT后常见的严重并发症之一,影响患者的预后和生存。 -
关键词:
- 再生障碍性贫血 /
- 单倍体造血干细胞移植 /
- EB病毒 /
- 淋巴增殖性疾病
Abstract:Objective To analyze the risk factors and survival status of Epstein-Barr virus (EBV) infection in patients with aplastic anemia (AA) after haploid allogeneic hematopoietic stem cell transplantation (Haplo-HSCT). Methods Clinical data of 78 AA patients who underwent Haplo-HSCT in the hematology department of a hospital from January 1, 2019 to October 31, 2022 were analyzed retrospectively. The occurrence and onset time of EBV viremia, EBV-related diseases (EBV diseases), and post-transplant lymphoproliferative disorders (PTLD) were observed, risk factors and survival status were analyzed. Results Among the 78 patients, 38 were males and 40 were females, with a median age of 33 (9-56) years old; 53 patients experienced EBV reactivation, with a total incidence of 67.9%, and the median time for EBV reactivation was 33 (13, 416) days after transplantation. Among patients with EBV reactivation, 49 cases (62.8%) were simple EBV viremia, 2 cases (2.6%) were possible EBV diseases, and 2 cases (2.6%) were already confirmed EBV diseases (PTLD). Univariate analysis showed that age 1 < 40 years old at the time of transplantation, umbilical cord blood infusion, occurrence of acute graft-versus-host disease(aGVHD) after transplantation, and concurrent cytomegalovirus (CMV) infection were independent risk factors for EBV reactivation in AA patients after Haplo-HSCT. Multivariate analysis showed that concurrent CMV infection was an independent risk factor for EBV reactivation in AA patients after Haplo-HSCT (P=0.048). Ritu-ximab intervention before stem cell reinfusion was a factor affecting the duration of EBV reactivation (P < 0.05). The mortality of EBV viremia, EBV diseases, and PTLD alone were 8.2%, 50.0%, and 100%, respectively. The 2-year overall survival rate of patients with and without EBV reactivation were 85.3%, and 90.7%, respectively, difference was not statistically significant (P=0.897). However, patients treated with rituximab had 2-year lower survival rate than those who did not use it, with a statistically significant difference (P=0.046). Conclusion EBV reactivation is one of the serious complications in AA patients after Haplo-HSCT, which affects the prognosis and survival of patients. -
再生障碍性贫血(aplastic anemia, AA)是临床常见的骨髓衰竭性疾病之一,其临床表现主要是贫血、出血和感染[1-2]。造血干细胞移植作为AA根治手段,显著提升了AA患者的生存率,且单倍体异基因造血干细胞移植(Haplo-HSCT)供者易获得,移植成功率高[3-5],但移植后EB病毒(EBV)再激活却严重影响患者的生存及生存质量[6-7]。目前AA Haplo-HSCT相关研究较少,为探究AA患者Haplo-HSCT后EBV再激活的危险因素及患者生存情况,本研究分析接受Haplo-HSCT的患者资料,了解EBV再激活相关情况与患者预后等因素的相关性,为临床早期防治AA异基因造血干细胞移植(allo-HSCT)患者EBV感染提供参考。
1. 对象与方法
1.1 研究对象
回顾性收集2019年1月1日—2022年10月31日某院83例进行Haplo-HSCT的AA患者临床资料,排除5例移植后早期(<2周)死亡患者。本研究最终纳入78例患者,其中男性38例,女性40例,中位年龄33(9~56)岁;非重型再生障碍性贫血(NSAA) 13例,重型再生障碍性贫血(SAA)65例,分型标准符合指南[8]。53例发生EBV再激活,其中单纯EBV血症49例,EBV病4例[包括移植后淋巴组织增殖性疾病(PTLD) 2例]。另外,14例患者因供者特异性抗体(DSA)阳性应用利妥昔单抗治疗。
1.2 预处理及移植物抗宿主病(GVHD)防治方案
全部患者均为亲缘单倍体移植,19例患者移植前预处理方案选择改良白消安/环磷酰胺(Bu/Cy)方案,即Bu 3.2 mg/kg·d×2 d+氟达拉滨(Flu) 30 mg/m2·d×5 d+Cy 50 mg/kg·d×4 d+抗胸腺细胞球蛋白(ATG) 2.5 mg/kg·d×4 d;59例患者移植前预处理方案选择FCA方案(即Flu、Cy、ATG),Flu 30 mg/m2·d×5 d+Cy 40~50 mg/kg·d×4 d+ATG 2.5 mg/kg·d×4 d。移植前DSA阳性处理方案:移植前11 d血浆置换、移植前10 d和3 d各应用利妥昔单抗375 mg/m2、移植当天和移植1 d后回输外周干细胞前各应用丙种球蛋白20 g。GVHD预防方案所有患者均选择环孢素(CsA)+短程甲氨蝶呤(MTX)+ 霉酚酸酯(MMF)方案,具体使用方法以及急性GVHD (aGVHD)诊断标准和分级参考最新版专家共识[9]。移植存活标准:中性粒细胞植入,连续3 d中性粒细胞绝对值(ANC) ≥0.5×109/L的第1天;血小板植入,连续7 d血小板计数≥20×109/L(脱离血小板输注)的第1天。
1.3 EBV感染分型及临床监测
临床EBV感染可分为三型,单纯EBV血症:检测到患者血液中存在EBV-DNA;可能的EBV疾病:可见明显的淋巴结病变(或其他内器官疾病)伴高EBV血负荷,无其他病因或已确诊疾病;已证实的EBV疾病(经病理确定的PTLD或其他器官内疾病):经活检或其他侵入性检查后通过病理从器官中检测到EBV,通常伴有器官受损的表现,主要是PTLD[10]。本中心所有患者从实施预处理方案起每周监测外周血全血EBV-DNA、巨细胞病毒(CMV)-DNA至移植后90 d,从移植后90 d起每两周监测一次直至移植后180 d,移植180 d后若出现疑似病毒感染的症状需复查EBV-DNA、CMV-DNA,同时,若监测到血EBV阳性,则继续每两周监测一次,直至病毒转阴。外周血全血EBV-DNA定量检测病毒载量>1×104连续3次则为阳性。
1.4 随访
对本研究纳入的所有患者采用门诊、住院或电话联系进行随访,随访终点为2022年10月31日,评估EBV再激活相关情况与患者预后等因素的相关性。
1.5 统计学方法
应用SPSS 25.0统计软件进行数据分析。采用χ2检验比较EBV感染发生率,采用Kaplan-Meier生存曲线进行生存分析计算生存率,采用COX回归对EBV感染相关风险进行单因素及多因素分析,以P≤0.05为差异有统计学意义。
2. 结果
2.1 EBV感染情况
78例患者中共有53例发生EBV感染,总发生率67.9%,EBV感染发生的中位时间为移植后33(13, 416) d,所有EBV感染患者中,单纯EBV血症49例(62.8%),可能的EBV疾病2例(2.6%),另外,已证实的EBV疾病(经病理确定的PTLD)2例(2.6%)。纳入患者中共有9例死亡,其中7例EBV再激活(4例因肺炎等重症感染死亡,1例因继发淋巴瘤累及中枢死亡,1例因继发代谢性脑病、持续癫痫大发作状态死亡,1例因重度aGVHD死亡),2例EBV未激活(1例因重症肺炎感染性休克继发心力衰竭死亡,1例因左侧额叶自发性脑出血死亡),总病死率为11.5%。单纯EBV血症患者共有4例死亡,病死率8.2%,可能的EBV疾病患者共有2例死亡,病死率50.0%,已证实的EBV疾病(经病理确定的PTLD)患者共有2例死亡,病死率100%。
2.2 EBV感染的危险因素分析
单因素分析提示移植时患者年龄<40岁、脐血辅助回输、移植后发生aGVHD、合并CMV感染是AA患者Haplo-HSCT后发生EBV感染的危险因素(均P<0.05)。女供男组与其他供受者性别组合方式组比较,差异无统计学意义,但两组激活率相差较大,因此将这两组也纳入多因素分析。多因素分析显示合并CMV再激活是移植后EBV感染的独立危险因素。见表 1。
表 1 AA患者进行Haplo-HSCT后EBV感染相关危险因素分析Table 1 Risk factors related to EBV infection in AA patients after Haplo-HSCT项目 全部(n=78,例) EBV激活[n=53,例(%)] EBV未激活[n=25,例(%)] 单因素分析 多因素分析 P HR(95%CI) P HR(95%CI) AA类型 0.091 0.206(0.029~0.441) - - NSAA 13 11(84.6) 2(15.4) SAA 50 32(64.0) 18(36.0) VSAA 15 10(66.7) 5(33.3) 移植时年龄[M(P25,P75),岁] 33(9,56) 32(9,56) 36(10,56) 0.033 0.250(0.012~0.488) 0.236 0.482(0.144~1.610) <40 56 42(75.0) 14(25.0) ≥40 22 11(50.0) 11(50.0) 受者性别 0.880 0.009(0.199~0.209) - - 男性 38 26(68.4) 12(31.6) 女性 40 27(67.5) 13(32.5) 供/受者性别 0.058 0.246(0.047~0.445) 0.077 0.220(0.041~1.176) 女供男 16 14(87.5) 2(12.5) 其他 62 39(62.9) 23(37.1) 供者受者血型相合度 0.514 0.300(0.047~0.647) - - 主不和 12 6(50.0) 6(50.0) 次不和 15 12(80.0) 3(20.0) 双向不和 5 3(60.0) 2(40.0) 相合 46 32(69.6) 14(30.4) 预处理方案 0.291 0.145(0.030~0.320) - - Bu/Cy 19 15(78.9) 4(21.1) FCA 59 38(64.4) 21(35.6) 脐血辅助回输 0.030 0.233(0.025~0.441) 0.139 2.352(0.758~7.299) 否 33 18(54.5) 15(45.5) 是 45 35(77.8) 10(22.2) 移植前受者EBV血清学 0.105 0.611(0.397~0.825) - 4.841(0.258~90.841) R- 3 3(100) 0(0) R+ 67 46(68.7) 21(31.3) 未知 8 4(50.0) 4(50.0) 移植前利妥昔单抗干预 0.902 0.132(0.149~0.413) - - 否 64 45(70.3) 19(29.7) 是 14 8(57.1) 6(42.9) 发生aGVHD 0.005 0.305(0.120~0.490) 0.077 3.288(0.280~12.281) 否 48 27(56.2) 21(43.8) 是 30 26(86.7) 4(13.3) 发生慢性GVHD (cGVHD) 0.055 0.185(0.074~0.296) - - 否 61 39(63.9) 22(36.1) 是 17 14(82.4) 3(17.6) 合并CMV再激活 0.004 0.308(0.119~0.497) 0.048 3.402(1.014~11.419) 否 44 24(54.5) 20(45.5) 是 34 29(85.3) 5(14.7) 注:-表示未进行分析;VSAA为极重型再生障碍性贫血。 2.3 EBV初次感染发生时间影响因素分析
单因素和多因素Cox回归分析均显示,干细胞回输前是否使用利妥昔单抗干预是EBV初次感染发生时间的影响因素,回输前使用利妥昔单抗的AA患者进行Haplo-HSCT后EBV再激活的时间推后,差异有统计学意义(P<0.05)。见表 2。
表 2 患者进行Haplo-HSCT后EBV初次感染时间影响因素的Cox回归分析模型Table 2 Cox regression analysis model of factors affecting the time of initial EBV infection in patients after Haplo-HSCT类别 病例数(n=53) EBV感染发生时间(移植后日数,d) 单因素分析 多因素分析 P HR(95%CI) P HR(95%CI) 移植时患者年龄(岁) 0.689 1.153(0.573~2.320) - - <40 42 44(20,279) ≥40 11 34(13,416) 受者性别 0.609 0.867(0.502~1.498) - - 男性 26 40(13,379) 女性 27 47(21,416) 供/受者性别 0.660 1.150(0.616~2.146) - - 女供男 14 41(13,379) 其他 39 39(20,416) 预处理方案 0.767 0.911(0.491~1.689) - - Bu/Cy 15 38(21,416) FCA 38 48(0,379) 脐血辅助回输 0.931 0.975(0.548~1.735) - - 否 18 43(13,367) 是 35 38(21,416) 移植前受者EBV血清学 0.228 1.505(0.448~5.056) - - R+ 46 48(13,416) R- 3 40(26,379) 未知 4 36(31,412) 移植前利妥昔单抗干预 0.005 0.285(0.118~0.688) 0.004 0.215(0.075~0.617) 否 45 42(13,367) 是 8 178(35,416) 发生aGVHD 0.106 0.628(0.357~1.105) - - 否 27 33(20,416) 是 26 35(13,379) 发生cGVHD 0.237 0.678(0.356~1.292) - - 否 39 40(13,379) 是 14 43(20,416) 合并CMV再激活 0.304 0.740(0.417~1.313) - - 否 24 43(23,283) 是 29 40(13,416) 注:R+:移植前受者EBV血清学阳性;R-:移植前受者EBV血清学阴性;-表示未进行分析。 2.4 EBV感染治疗
EBV感染临床上常规应用抗病毒药物诸如更昔洛韦、磷甲酸治疗,本研究患者2周的病毒转阴率20.8%,除此之外,14例患者在allo-HSCT中使用利妥昔单抗(375 mg/m2/qw)治疗,与64例未使用利妥昔单抗治疗患者生存时间进行Kaplan-Meier分析,结果表明后者累积生存率高于前者,差异有统计学意义(P=0.046)。见图 1。
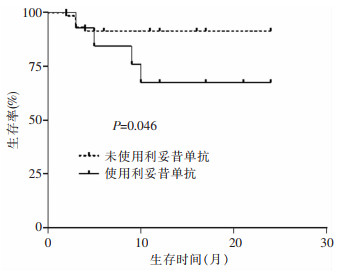 图 1 移植前使用利妥昔单抗干预和未使用利妥昔单抗干预总生存率比较Fig. 1 Comparison of overall survival rates between patients with and without rituximab intervention before transplantation
图 1 移植前使用利妥昔单抗干预和未使用利妥昔单抗干预总生存率比较Fig. 1 Comparison of overall survival rates between patients with and without rituximab intervention before transplantation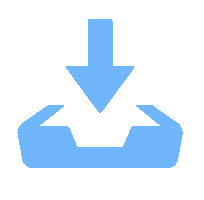 下载:
全尺寸图片
下载:
全尺寸图片
2.5 EBV感染后患者生存分析
EBV再激活患者2年生存率为85.3%,EBV未激活患者2年生存率为90.7%,差异无统计学意义(P=0.897)。见图 2。纳入移植时患者年龄、供受者性别、脐血辅助回输情况、aGVHD发生情况、cGVHD发生情况、合并CMV感染与否构建多因素Cox比例风险模型,结果显示:移植后合并CMV再激活对生存时间的影响具有统计学意义[HR=3.402, 95%CI(1.014~11.419),P=0.048],其他变量对生存时间的影响无统计学意义。
 图 2 EBV再激活和EBV未激活患者总生存率比较Fig. 2 Comparison of overall survival rates between EBV reactivated and EBV non-reactivated patients下载:
全尺寸图片
图 2 EBV再激活和EBV未激活患者总生存率比较Fig. 2 Comparison of overall survival rates between EBV reactivated and EBV non-reactivated patients下载:
全尺寸图片
3. 讨论
EBV再激活是困扰AA患者Haplo-HSCT的严重并发症之一,严重影响患者的生存和生活质量。本研究表明,AA患者Haplo-HSCT后EBV再激活的累积发生率为67.9%,略高于既往文献18.8%~44.1%的研究结果[11-13],可能与AA本身是免疫性疾病,并且移植过程中应用大剂量ATG及长时间应用钙调磷酸酶抑制剂(CNI)造成移植后免疫重建相对较晚相关[14]。本研究显示移植时患者年龄<40岁、脐血辅助回输、移植后发生aGVHD、合并CMV感染是AA患者Haplo-HSCT后发生EBV再激活的独立危险因素,而合并CMV感染则是其多因素分析中唯一的独立危险因素。其中脐血辅助回输、移植后发生aGVHD、合并CMV感染的AA患者进行Haplo-HSCT后EBV再激活率更高,与既往文献[11, 15]报道结果一致。但本研究显示年龄<40岁的患者EBV再激活率更高,可能与本研究中患者年龄的分布偏倚相关。
移植后患者处于免疫应答抑制状态,EBV极易激活,其可借助自身的外包膜糖蛋白gp350/220与B淋巴细胞膜上表达丰富的CR2结合,从而侵入B淋巴细胞[16-17],导致EBV相关的PTLD和其他EBV疾病,影响患者的生存。研究中EBV再激活患者中单纯EBV血症49例(62.8%),可能的EBV病2例(2.6%)和2例(2.6%)已确定的EBV病—PTLD患者。本研究显示EBV再激活的患者的2年生存率为85.3%,低于EBV未激活患者的2年生存率(90.7%),提示EBV再激活可对移植后患者生存产生影响。EBV再激活患者的总病死率为11.5%,低于相关文献报道的血液病患者移植后EBV再激活患者病死率(32.4%)[18]。单纯EBV血症病死率为8.2%,EBV病病死率为50.0%,而PTLD病死率高达100%,提示随着EBV再激活后的发生和发展,其导致患者病死率显著增加,PTLD尤甚[19],PTLD是Haplo-HSCT后罕见但可能致命的并发症,主要危险因素是移植物的T细胞耗损(TCD)、不匹配或无亲缘关系的供体(URD)、脐血移植及AA移植因素等[20]。因此,如何降低EBV再激活以及规范的抢先治疗显得尤为重要。
本研究将可能影响EBV初次激活时间的变量纳入Cox回归分析,单因素和多因素分析均表明,移植前使用利妥昔单抗的AA患者进行Haplo-HSCT后EBV再激活的时间更晚。移植后患者EBV再激活后导致B细胞增殖,而利妥昔单抗作为抗CD20单克隆抗体,其可以通过抗体依赖的细胞毒作用、补体依赖细胞毒作用和诱导凋亡等机制发挥清除CD20阳性的B淋巴细胞[21],以此起到对患者体内EBV病毒的清除作用。对于血清EBV病毒载量较高的患者指南建议预防性使用利妥昔单抗抢先治疗[10],但同时由此会引发正常B淋巴细胞数量减低,进而导致移植后供者来源B细胞重建延迟,造成免疫功能缺陷,增加了发生严重感染的概率[22-24]。本研究显示利妥昔单抗组EBV再激活率降低,但整体生存率却偏低,考虑与继发严重感染有关[25]。
总之,AA患者进行Haplo-HSCT后EBV再激活发生率高,而利妥昔单抗早期干预又增加感染和死亡风险,因此,需早期识别EBV再激活高危因素并规律EBV-DNA拷贝数监测,抢先治疗EBV再激活,尽可能降低其相关病死率,改善患者预后。本研究结果需进一步扩大样本且进行多中心前瞻性研究验证。
利益冲突:所有作者均声明不存在利益冲突。
-
图 1 移植前使用利妥昔单抗干预和未使用利妥昔单抗干预总生存率比较
Fig. 1 Comparison of overall survival rates between patients with and without rituximab intervention before transplantation
下载:
全尺寸图片
图 2 EBV再激活和EBV未激活患者总生存率比较
Fig. 2 Comparison of overall survival rates between EBV reactivated and EBV non-reactivated patients
下载:
全尺寸图片
表 1 AA患者进行Haplo-HSCT后EBV感染相关危险因素分析
Table 1 Risk factors related to EBV infection in AA patients after Haplo-HSCT
项目 全部(n=78,例) EBV激活[n=53,例(%)] EBV未激活[n=25,例(%)] 单因素分析 多因素分析 P HR(95%CI) P HR(95%CI) AA类型 0.091 0.206(0.029~0.441) - - NSAA 13 11(84.6) 2(15.4) SAA 50 32(64.0) 18(36.0) VSAA 15 10(66.7) 5(33.3) 移植时年龄[M(P25,P75),岁] 33(9,56) 32(9,56) 36(10,56) 0.033 0.250(0.012~0.488) 0.236 0.482(0.144~1.610) <40 56 42(75.0) 14(25.0) ≥40 22 11(50.0) 11(50.0) 受者性别 0.880 0.009(0.199~0.209) - - 男性 38 26(68.4) 12(31.6) 女性 40 27(67.5) 13(32.5) 供/受者性别 0.058 0.246(0.047~0.445) 0.077 0.220(0.041~1.176) 女供男 16 14(87.5) 2(12.5) 其他 62 39(62.9) 23(37.1) 供者受者血型相合度 0.514 0.300(0.047~0.647) - - 主不和 12 6(50.0) 6(50.0) 次不和 15 12(80.0) 3(20.0) 双向不和 5 3(60.0) 2(40.0) 相合 46 32(69.6) 14(30.4) 预处理方案 0.291 0.145(0.030~0.320) - - Bu/Cy 19 15(78.9) 4(21.1) FCA 59 38(64.4) 21(35.6) 脐血辅助回输 0.030 0.233(0.025~0.441) 0.139 2.352(0.758~7.299) 否 33 18(54.5) 15(45.5) 是 45 35(77.8) 10(22.2) 移植前受者EBV血清学 0.105 0.611(0.397~0.825) - 4.841(0.258~90.841) R- 3 3(100) 0(0) R+ 67 46(68.7) 21(31.3) 未知 8 4(50.0) 4(50.0) 移植前利妥昔单抗干预 0.902 0.132(0.149~0.413) - - 否 64 45(70.3) 19(29.7) 是 14 8(57.1) 6(42.9) 发生aGVHD 0.005 0.305(0.120~0.490) 0.077 3.288(0.280~12.281) 否 48 27(56.2) 21(43.8) 是 30 26(86.7) 4(13.3) 发生慢性GVHD (cGVHD) 0.055 0.185(0.074~0.296) - - 否 61 39(63.9) 22(36.1) 是 17 14(82.4) 3(17.6) 合并CMV再激活 0.004 0.308(0.119~0.497) 0.048 3.402(1.014~11.419) 否 44 24(54.5) 20(45.5) 是 34 29(85.3) 5(14.7) 注:-表示未进行分析;VSAA为极重型再生障碍性贫血。 表 2 患者进行Haplo-HSCT后EBV初次感染时间影响因素的Cox回归分析模型
Table 2 Cox regression analysis model of factors affecting the time of initial EBV infection in patients after Haplo-HSCT
类别 病例数(n=53) EBV感染发生时间(移植后日数,d) 单因素分析 多因素分析 P HR(95%CI) P HR(95%CI) 移植时患者年龄(岁) 0.689 1.153(0.573~2.320) - - <40 42 44(20,279) ≥40 11 34(13,416) 受者性别 0.609 0.867(0.502~1.498) - - 男性 26 40(13,379) 女性 27 47(21,416) 供/受者性别 0.660 1.150(0.616~2.146) - - 女供男 14 41(13,379) 其他 39 39(20,416) 预处理方案 0.767 0.911(0.491~1.689) - - Bu/Cy 15 38(21,416) FCA 38 48(0,379) 脐血辅助回输 0.931 0.975(0.548~1.735) - - 否 18 43(13,367) 是 35 38(21,416) 移植前受者EBV血清学 0.228 1.505(0.448~5.056) - - R+ 46 48(13,416) R- 3 40(26,379) 未知 4 36(31,412) 移植前利妥昔单抗干预 0.005 0.285(0.118~0.688) 0.004 0.215(0.075~0.617) 否 45 42(13,367) 是 8 178(35,416) 发生aGVHD 0.106 0.628(0.357~1.105) - - 否 27 33(20,416) 是 26 35(13,379) 发生cGVHD 0.237 0.678(0.356~1.292) - - 否 39 40(13,379) 是 14 43(20,416) 合并CMV再激活 0.304 0.740(0.417~1.313) - - 否 24 43(23,283) 是 29 40(13,416) 注:R+:移植前受者EBV血清学阳性;R-:移植前受者EBV血清学阴性;-表示未进行分析。 -
[1] Furlong E, Carter T. Aplastic anaemia: current concepts in diagnosis and management[J]. J Paediatr Child Health, 2020, 56(7): 1023-1028. doi: 10.1111/jpc.14996 [2] Patel BJ, Barot SV, Kuzmanovic T, et al. Distinctive and common features of moderate aplastic anaemia[J]. Br J Haematol, 2020, 189(5): 967-975. doi: 10.1111/bjh.16460 [3] Zhang XH, Chen J, Han MZ, et al. The consensus from The Chinese Society of Hematology on indications, conditioning regimens and donor selection for allogeneic hematopoietic stem cell transplantation: 2021 update[J]. J Hematol Oncol, 2021, 14(1): 145. doi: 10.1186/s13045-021-01159-2 [4] Xu LP, Xu ZL, Wang SQ, et al. Long-term follow-up of haploidentical transplantation in relapsed/refractory severe aplastic anemia: a multicenter prospective study[J]. Sci Bull (Beijing), 2022, 67(9): 963-970. doi: 10.1016/j.scib.2022.01.024 [5] Lin F, Han TT, Zhang YY, et al. The incidence, outcomes, and risk factors of secondary poor graft function in haploidentical hematopoietic stem cell transplantation for acquired aplastic anemia[J]. Front Immunol, 2022, 13: 896034. doi: 10.3389/fimmu.2022.896034 [6] Annaloro C, Serpenti F, Saporiti G, et al. Viral infections in HSCT: detection, monitoring, clinical management, and immunologic implications[J]. Front Immunol, 2020, 11: 569381. [7] Zhou JR, Shi DY, Wei R, et al. Co-reactivation of Cytomegalovirus and Epstein-Barr virus was associated with poor prognosis after allogeneic stem cell transplantation[J]. Front Immunol, 2021, 11: 620891. doi: 10.3389/fimmu.2020.620891 [8] 中华医学会血液学分会红细胞疾病(贫血)学组. 再生障碍性贫血诊断与治疗中国指南(2022年版)[J]. 中华血液学杂志, 2022, 43(11): 881-888. Red Blood Cell Disease(Anemia) Group, Chinese Society of Hematology, Chinese Medical Association. Guidelines for the diagnosis and management of aplastic anemia in China (2022)[J]. Chinese Journal of Hematology, 2022, 43(11): 881-888. [9] 中华医学会血液学分会干细胞应用学组. 中国异基因造血干细胞移植治疗血液系统疾病专家共识(Ⅲ)——急性移植物抗宿主病(2020年版)[J]. 中华血液学杂志, 2020, 41(7): 529-536. Stem Cell Application Group, Chinese Society of Hematology, Chinese Medical Association. Chinese consensus of allogeneic hematopoietic stem cell transplantation for hematological disease (Ⅲ) —acute graft-versus-host disease (2020)[J]. Chinese Journal of Hematology, 2020, 41(7): 529-536. [10] Styczynski J, Tridello G, Wendel L, et al. Prevalence, management, and new treatment modalities of EBV-DNA-emia and EBV-PTLD after allo-HCT: survey of infectious diseases working party EBMT[J]. Bone Marrow Transplant, 2024, 59(1): 59-65. doi: 10.1038/s41409-023-02129-7 [11] Gao XN, Lin J, Wang LJ, et al. Risk factors and clinical outcomes of Epstein-Barr virus DNAemia and post-transplant lymphoproliferative disorders after haploidentical and matched-sibling PBSCT in patients with hematologic malignancies[J]. Ann Hematol, 2019, 98(9): 2163-2177. doi: 10.1007/s00277-019-03742-7 [12] Wang H, Zhang TT, Qi JQ, et al. Incidence, risk factors, and clinical significance of Epstein-Barr virus reactivation in myelodysplastic syndrome after allogeneic haematopoietic stem cell transplantation[J]. Ann Hematol, 2019, 98(4): 987-996. doi: 10.1007/s00277-019-03603-3 [13] Zhou L, Gao ZY, Lu DP. Incidence, risk factors, and clinical outcomes associated with Epstein-Barr virus-DNAemia and Epstein-Barr virus-associated disease in patients after haploidentical allogeneic stem cell transplantation: a single-center study[J]. Clin Transplant, 2020, 34(6): e13856. doi: 10.1111/ctr.13856 [14] Maeda Y. Immune reconstitution after T-cell replete HLA haploidentical hematopoietic stem cell transplantation using high-dose post-transplant cyclophosphamide[J]. J Clin Exp Hematop, 2021, 61(1): 1-9. doi: 10.3960/jslrt.20040 [15] 李群, 毛晓蕾, 邱婷婷, 等. 异基因造血干细胞移植后EB病毒感染的临床分析[J]. 徐州医科大学学报, 2021, 41(8): 554-558. Li Q, Mao XL, Qiu TT, et al. Clinical analysis of Epstein Barr virus infection after allogeneic hematopoietic stem cell transplantation[J]. Journal of Xuzhou Medical University, 2021, 41(8): 554-558. [16] Liang JH, Wang C, Yiu SPT, et al. Epstein-Barr virus induced cytidine metabolism roles in transformed B-cell growth and survival[J]. mBio, 2021, 12(4): e0153021. doi: 10.1128/mBio.01530-21 [17] Yu H, Robertson ES. Epstein-Barr virus history and pathogenesis[J]. Viruses, 2023, 15(3): 714. doi: 10.3390/v15030714 [18] Ding YY, Ru YH, Song TM, et al. Epstein-Barr virus and Cytomegalovirus reactivation after allogeneic hematopoietic cell transplantation in patients with non-Hodgkin lymphoma: the prevalence and impacts on outcomes[J]. Ann Hematol, 2021, 100(11): 2773-2785. doi: 10.1007/s00277-021-04642-5 [19] Al Hamed R, Bazarbachi AH, Mohty M. Epstein-Barr virus-related post-transplant lymphoproliferative disease (EBV-PTLD) in the setting of allogeneic stem cell transplantation: a comprehensive review from pathogenesis to forthcoming treatment modalities[J]. Bone Marrow Transplant, 2020, 55(1): 25-39. doi: 10.1038/s41409-019-0548-7 [20] García-Cadenas I, Yáñez L, Jarque I, et al. Frequency, characteristics, and outcome of PTLD after allo-SCT: a multicenter study from the Spanish group of blood and marrow transplantation (GETH)[J]. Eur J Haematol, 2019, 102(6): 465-471. doi: 10.1111/ejh.13226 [21] 全国儿童EB病毒感染协作组, 中华实验和临床病毒学杂志编辑委员会. EB病毒感染实验室诊断及临床应用专家共识[J]. 中华实验和临床病毒学杂志, 2018, 32(1): 2-8. National EB Virus Infection Collaboration Group for Children, Editorial Board of Chinese Journal of Experimental and Clinical Virology. Expert consensus on laboratory diagnosis and clinical application of Epstein-Barr virus infection[J]. Chinese Journal of Experimental and Clinical Virology, 2018, 32(1): 2-8. [22] Romero S, Montoro J, Guinot M, et al. Post-transplant lymphoproliferative disorders after solid organ and hematopoietic stem cell transplantation[J]. Leuk Lymphoma, 2019, 60(1): 142-150. [23] Athni TS, Barmettler S. Hypogammaglobulinemia, late-onset neutropenia, and infections following rituximab[J]. Ann Allergy Asthma Immunol, 2023, 130(6): 699-712. [24] Ottaviano G, Sgrulletti M, Moschese V. Secondary rituximab-associated versus primary immunodeficiencies: the enigmatic border[J]. Eur J Immunol, 2022, 52(10): 1572-1580. [25] Kao RL, Holtan SG. Host and graft factors impacting infection risk in hematopoietic cell transplantation[J]. Infect Dis Clin North Am, 2019, 33(2): 311-329.
