
Risk factors of central line-associated bloodstream infection in the intensive care unit based on propensity score matching
-
摘要:
目的 探讨中心静脉导管相关血流感染(CLABSI)的独立危险因素, 为制定感染防控的干预措施和开展针对性治疗提供依据。 方法 回顾性收集2019年1月—2023年12月某院诊断为CLABSI的患者, 将其定义为感染组, 并采用倾向性评分匹配(PSM)法1 ∶4匹配置入中心静脉导管(CVC)且未发生感染的患者为对照组。以是否发生CLABSI为因变量, 将匹配后两组的可能危险因素为自变量进行logistic回归分析, 探索患者发生CLABSI的独立危险因素。 结果 共匹配CLABSI组患者42例, 非CLABSI组患者168例。多因素logistic回归分析显示, 急性生理学及慢性健康状况(APACHE Ⅱ)评分高[OR=1.217, 95%CI(1.094~1.357), P<0.001]、中心静脉置管时间长[OR=1.273, 95%CI(1.157~1.400), P<0.001]及股静脉置管[OR=6.846, 95%CI(1.511~31.014), P=0.013]是CLABSI发生的独立危险因素。42例CLABSI患者共分离病原菌118株, 以革兰阴性菌为主(56株)。 结论 高APACHE Ⅱ评分、中心静脉置管时间长及股静脉置管是CLABSI发生的独立危险因素, 主要病原菌为革兰阴性杆菌, 针对这些危险因素严格落实CLABSI相应的防控措施, 减少感染风险。 -
关键词:
- 中心静脉导管相关血流感染 /
- 中心静脉导管 /
- 倾向性评分匹配 /
- 危险因素 /
- CLABSI
Abstract:Objective To explore the independent risk factors for central line-associated bloodstream infection (CLABSI), provide basis for developing intervention measures for infection prevention and control as well as conducting targeted treatment. Methods Patients who were diagnosed with CLABSI in a hospital from January 2019 to December 2023 were recruited retrospectively and defined as the infection group. According to 1 ∶4 propensity score matching method, patients who received central venous catheter (CVC) without infection were taken as the control group. With whether CLABSI occurred as the dependent variable, the possible risk factors of the matched two groups as the independent variables, logistic regression analysis was conducted, and independent risk factors for patients developing CLABSI were explored. Results A total of 42 patients in the CLABSI group and 168 patients in the non-CLABSI group were matched. Multivariate logistic regression analysis showed that high score of acute physiology and chronic health evaluation (APACHE) Ⅱ (OR=1.217, 95%CI [1.094-1.357], P < 0.001), long duration of central venous catheterization (OR=1.273, 95%CI [1.157-1.400], P < 0.001), and femoral venous catheterization (OR=6.846, 95%CI [1.511-31.014], P=0.013) were independent risk factors for CLABSI. A total of 118 strains of pathogens were isolated from 42 CLABSI patients, with Gram-negative bacteria being the majority (n=56). Conclusion High score of APACHE Ⅱ, long duration of central venous catheterization, and femoral venous catheterization are independent risk factors for CLABSI. The main pathogens are Gram-negative bacilli. Strict prevention and control measures for CLABSI should be implemented to reduce the risk of infection. -
在成人重症监护病房(intensive care unit, ICU)中,中心静脉导管(central venous catheter, CVC)的使用对治疗病情复杂的患者至关重要。虽然CVC可为患者带来潜在益处,但发生导管相关血流感染(central line-associated bloodstream infection, CLABSI)仍然是中心静脉通路最严重的并发症,也是ICU医院感染的主要原因[1]。因此,早期识别CLABSI发生的独立危险因素并分析病原菌特点,是实施有效预防与控制措施和开展针对性治疗的前提。CLABSI的危险因素较多,研究[2-3]表明,患者年龄>60岁、男性、糖尿病均是CLABSI发生的危险因素;但另一项研究中,糖尿病与CLABSI发生率降低相关[OR=0.63;95%CI(0.45~0.88)][4];还有研究[5]显示患者年龄、性别、患病情况等均与CLABSI无显著相关性。不同研究可能存在偏倚等问题,影响研究结果,导致结果存在异质性,因此平衡病例和对照之间的基线特征控制偏倚至关重要。
采用倾向评分匹配(propensity score mat-ching, PSM)方法,感染组和对照组具有相似的测量基线协变量分布,做出的有关危险因素的推论有效,结果更真实可信[6]。本研究采用PSM法来平衡病例组和对照组患者的年龄、性别、患病情况等基线临床资料,分析置管后ICU患者发生CLABSI的独立危险因素。
1. 对象与方法
1.1 研究对象
回顾性收集2019年1月—2023年12月泰州市某三级甲等医院医院感染管理处医院感染监测杏林系统中诊断为CLABSI的患者,将其定义为感染组,以《血管内导管相关感染的预防与治疗指南》为感染诊断标准[7]。确定感染组后,采用PSM法匹配置入CVC且未发生感染的患者为对照组。
1.2 研究方法
为进一步探索患者CVC置管后发生CLABSI的独立危险因素,采用PSM法,将两组患者资料中的年龄、性别、糖尿病史、高血压史、恶性肿瘤、心功能不全、肾功能不全共7个协变量进行1∶4配对匹配,即采用倾向指数无放回卡钳匹配法均衡组间的基线,卡钳值设为0.05。标准化均差(standardized mean difference, SMD)用于评估组间匹配后的平衡,SMD<0.1表明平衡性较好[6]。
以是否发生CLABSI为因变量,将急性生理学及慢性健康状况评分系统(acute physiology and chronic health evaluation, APACHE Ⅱ)评分、CVC置管时间、置管位置(颈内静脉、锁骨下静脉、股静脉)、手术史(0=无,1=有)、使用抗菌药物(0=否,1=是)、联合使用抗菌药物(0=否,1=是)、呼吸机使用(0=否,1=是)、导尿管置管(0=否,1=是)、白细胞计数(0=正常值组,1=异常值组)、中性粒细胞计数(0=正常值组,1=异常值组)、C反应蛋白(0=正常值组,1=异常值组)共11个协变量为自变量进行logistic回归分析。
1.3 细菌鉴定与药敏试验
采用VITEK-MS全自动微生物鉴定仪进行病原学鉴定,采用VITEK 2 Compact及配套的AST-GP67、AST-N335、AST-XN04药敏板进行药敏试验。
1.4 统计分析
应用R 4.3.2软件进行PSM,应用SPSS 24.0进行统计学分析。计量资料采用均数±标准差表示,采用t检验进行比较;计数资料采用例(%)表示,采用卡方检验进行比较;多因素分析采用logistic逐步回归分析;P≤0.05为差异有统计学意义。
2. 结果
2.1 匹配前后两组患者一般资料比较
共选取2019年1月—2023年12月诊断为CLABSI的患者44例,为感染组,95.45%的感染组病例经PSM法匹配成功,最终纳入感染组42例和对照组168例。2019—2013年CLABSI发病率为1.10‰(44/40 057)。匹配前两组患者的糖尿病、心功能不全、肾功能不全等情况比较,差异均有统计学意义(均P<0.05),且有多项协变量SMD值>0.1,不具有可比性。匹配后两组患者一般资料比较,除年龄略>0.1,其余变量SMD值均<0.1,并且采用PSM后7个协变量在组间分布的P值均>0.05,表明两个组别之间的协变量平衡得到改善。均衡性较好,见表 1。
表 1 匹配前后两组患者基本临床资料Table 1 Baseline characteristics of two groups of patients before and after matching基本资料 匹配前 t/χ2 P SMD 匹配后 t/χ2 P SMD 感染组(n=44) 非感染组(n=4 366) 感染组(n=42) 对照组(n=168) 年龄(x±s,岁) 65.09±15.07 66.29±15.43 0.51 0.609 -0.079 65.38±15.34 67.45±15.39 0.78 0.436 -0.118 性别[例(%)] 1.66 0.198 0.186 0.61 0.433 0.012 男 24(54.5) 2 791(63.9) 24(57.1) 107(63.7) 女 20(45.5) 1 575(36.1) 18(42.9) 61(36.3) 糖尿病[例(%)] 15.09 < 0.001 0.509 0.70 0.401 -0.024 有 22(50.0) 1 073(24.6) 20(47.6) 68(40.5) 无 22(50.0) 3 293(75.4) 22(52.4) 100(59.5) 高血压[例(%)] 2.49 0.114 0.246 0.12 0.727 0.004 有 27(61.4) 2 157(49.4) 25(59.5) 95(56.5) 无 17(38.6) 2 209(50.6) 17(40.5) 73(43.5) 恶性肿瘤[例(%)] 0.03 0.868 -0.026 <0.01 1.000 0.087 有 6(13.6) 634(14.5) 5(11.9) 20(11.9) 无 38(86.4) 3 732(85.5) 37(88.1) 148(88.1) 心功能不全[例(%)] 15.77 <0.001 -0.603 - - <0.001 有 0(0) 1 155(26.5) 0(0) 0(0) 无 44(100) 3 211(73.5) 42(100) 168(100) 肾功能不全[例(%)] 8.91 0.003 0.454 0.18 0.676 -0.049 有 27(61.4) 1 714(39.3) 25(59.5) 94(56.0) 无 17(38.6) 2 652(60.7) 17(40.5) 74(44.0) 2.2 倾向评分的分布情况
图 1中的圆圈代表样本,横坐标指代倾向评分,底部为未匹配的对照组样本。未匹配的对照组样本多为倾向评分得分低的单元。匹配后,中间两组感染组和对照组评分趋于接近,符合预期。匹配后,感染组与对照组之间的倾向评分的分布更加接近,匹配效果较好,见图 2。
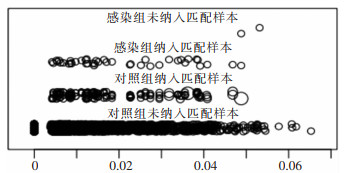 图 1 倾向评分的分布图Fig. 1 Distribution of propensity score
图 1 倾向评分的分布图Fig. 1 Distribution of propensity score 下载:
全尺寸图片
下载:
全尺寸图片
 图 2 倾向评分分布直方图注:AC为未匹配的直方图;BD为匹配后的直方图。Fig. 2 Histogram of propensity score distribution下载:
全尺寸图片
图 2 倾向评分分布直方图注:AC为未匹配的直方图;BD为匹配后的直方图。Fig. 2 Histogram of propensity score distribution下载:
全尺寸图片
2.3 CLABSI病原菌分布
42例感染组患者中共分离出病原菌118株,以革兰阴性菌为主(56株,占47.4%),主要为肺炎克雷伯菌(14.4%)、大肠埃希菌(11.0%)、鲍曼不动杆菌(8.5%)。革兰阳性菌52株(占44.1%),以金黄色葡萄球菌为主(11.9%),其次是表皮葡萄球菌(8.5%)。肺炎克雷伯菌、金黄色葡萄球菌和大肠埃希菌是引起CLABSI前三位的病原菌,见表 2。
表 2 CLABSI病原体分布情况Table 2 Distribution of pathogens causing CLABSI病原体 菌株数 构成比(%) 革兰阳性菌 52 44.1 金黄色葡萄球菌 14 11.9 表皮葡萄球菌 10 8.5 人葡萄球菌 9 7.6 肠球菌 8 6.8 头状葡萄球菌 8 6.8 溶血葡萄球 3 2.5 革兰阴性菌 56 47.4 肺炎克雷伯菌 17 14.4 大肠埃希菌 13 11.0 鲍曼不动杆菌 10 8.5 铜绿假单胞菌 9 7.6 阴沟肠杆菌 7 5.9 真菌 10 8.5 白念珠菌 10 8.5 合计 118 100 2.4 CLABSI影响因素单因素分析
匹配基本临床资料后,对ICU患者进行CLABSI影响因素的单因素分析,结果显示中心静脉置管时间、APACHE Ⅱ评分、置管部位、抗菌药物使用、联合使用抗菌药物、C反应蛋白异常比例6个因素比较,差异均有统计学意义(均P<0.05),见表 3。
表 3 匹配后两组患者CLABSI影响因素的单因素分析Table 3 Univariate analysis on the influencing factors for CLABSI in two groups of patients after matching因素 感染组(n=42) 对照组(n=168) t/χ2 P 因素 感染组(n=42) 对照组(n=168) t/χ2 P 中心静脉置管时间(x±s,d) 31.00±23.82 6.43±5.90 -14.24 <0.001 手术史[例(%)] 0.450 0.504 是 27(64.3) 117(69.6) APACHE Ⅱ评分(x±s,分) 27.55±8.37 20.84±5.85 -6.042 <0.001 否 15(35.7) 51(30.4) 使用呼吸机[例(%)] 2.470 0.115 是 11(26.2) 66(39.3) 置管部位[例(%)] 23.700 <0.001 否 31(73.8) 102(60.7) 颈内静脉 10(23.8) 89(53.0) 导尿管置管[例(%)] 0.214 0.643 锁骨下静脉 6(14.3) 40(23.8) 是 8(19.0) 27(16.1) 股静脉 26(61.9) 39(23.2) 否 34(81.0) 141(83.9) 使用抗菌药物[例(%)] 13.130 <0.001 白细胞计数[例(%)] 0.481 0.488 正常值组 17(40.5) 78(46.4) 是 42(100) 126(75.0) 异常值组 25(59.5) 90(53.6) 中性粒细胞计数[例(%)] 0.583 0.445 否 0(0) 42(25.0) 联合使用抗菌药物[例(%)] 10.683 0.001 正常值组 10(23.8) 50(29.8) 异常值组 32(76.2) 118(70.2) ≤2种 9(21.4) 83(49.4) C反应蛋白[例(%)] 5.241 0.022 正常值组 5(11.9) 49(29.2) ≥3种 33(78.6) 85(50.6) 异常值组 37(88.1) 119(70.8) 注:白细胞计数正常值为(3.5~9.5)×109/L;中性粒细胞计数正常值为(1.8~6.3)×109/L;C反应蛋白参考范围0~10 mg/L。 2.5 CLABSI影响因素的logistic回归分析
以是否发生CLABSI作为因变量(未发生CLABSI=0,发生CLABSI=1),以匹配后单因素分析有统计学意义的项目为自变量,进行logistic回归分析。APACHE Ⅱ评分高[OR=1.217,95%CI(1.091~1.357),P<0.001]、中心静脉置管时间长[OR=1.273,95%CI(1.157~1.400),P<0.001],股静脉置管[OR=6.846,95%CI(1.511~31.014),P=0.013]是患者发生CLABSI的独立危险因素,见表 4。
表 4 匹配后两组患者CLABSI多因素logistic回归分析Table 4 Multivariate logistic regression analysis on CLABSI in two groups of patients after matching因素 β Waldχ2 P OR 95%CI APACHE Ⅱ评分 0.196 12.478 <0.001 1.217 1.091~1.357 中心静脉置管时间 0.241 24.464 <0.001 1.273 1.157~1.400 颈内静脉置管(参照组) - 9.581 0.008 - - 锁骨下静脉置管 -0.409 0.197 0.657 0.664 0.109~4.036 股静脉置管 1.924 6.228 0.013 6.846 1.511~31.014 常量 -29.742 0 0.995 - - 注:-表示无数据。 3. 讨论
PSM是一种非随机对照研究常用的统计方法,能消除随机化分组研究中的混杂偏差,广泛应用于统计、医学和社会科学文献中[6]。PSM是由Rosenbaum和Rubin在1983年首次提出的一种非随机化研究的新方法,可以控制影响因素在组间分布的不均衡,可以最小化混杂偏倚,增加组间对比的均衡性,使研究因素更具有真实性[8]。近年来国内外应用PSM进行危险因素的研究逐渐增多,但是目前将其应用于CLABSI危险因素的分析较少见。本研究感染组和对照组的样本量差别较大,为尽可能保留原样本的信息,采用1∶4匹配,因为相关研究结果显示在某些情况下,1∶n匹配可以更好的减少估计的偏倚[9]。本研究通过PSM匹配两组患者临床基本资料后,分析2019—2023年与CLABSI相关的独立危险因素,两组之间的基线特征平衡且具有可比性。分析结果显示,CLABSI相关危险因素为高APACHE Ⅱ评分、中心静脉置管时间长和股静脉置管,检出病原菌革兰阳性菌52株,革兰阴性菌56株,真菌10株。
ICU患者发生CLABSI的风险较高,由于频繁置入一种或者多种导管,尤其紧急置入无菌操作未实施到位的情况下导致感染风险更高。阿曼2所三级医院ICU的CLABSI相关危险因素研究显示,CLABSI发病率均超过8例/1 000导管日[10]。本文未匹配前CLABSI发病率为1.10‰,处于较低水平;高于吕倩等[11]的研究,采取精细化防控措施干预前CLABSI发病率为0.15‰,说明针对CLABSI发生危险因素采取干预措施,对预防感染有效。低于相关研究结果(CLABSI发病率分别为3.12‰[12]、2.46‰[13]),可能与该院更加重视医院感染防控工作,增加感染防控投入,每周对ICU“三管”进行督查有关。
本研究中CLABSI患者导管置管平均持续时间为31 d,远高于非CLABSI组的6.43 d,与国外的一项研究[14]结果类似,ICU CLABSI患者的平均导管置管时间25.3 d,而未感染的ICU置管患者的平均导管置管时间为8.8 d。研究[15-16]均表明,导管留置时间越长发生CLABSI的风险越高;杨婷等[17]研究量化CLABSI死亡风险比发现,置管时间>7 d的患者发生死亡的风险是≤7 d的49倍;李元叶等[18]研究报道ICU置管时间>14 d的患者发生CLABSI的风险是置管时间<14 d的6.3倍。细菌生长繁殖与迁移需要一定的时间,患者血管导管留置越久,定植在导管上的细菌被带进血液的机会就越大,细菌繁殖越多,进入血液的细菌量就越多,从而导致CLABSI的发生[12]。临床医生需要避免不必要的导管置管,并及时拔除不再需要的CVC[19]。
APACHE Ⅱ评分使用基于12项常规生理测量初始值、年龄和既往健康状况评分评估疾病严重程度的一般衡量标准,0~71分,得分越高,病情越严重[20]。本文APACHE Ⅱ分值是由ICU质控医生对ICU患者入科24 h内进行评分,其中感染组的APACHE Ⅱ分值为(27.55±8.37)分,高于对照组的(20.84±5.85)分,差异具有统计学意义(P<0.001)。研究[1]显示APACHE Ⅱ评分>20分是发生CLABSI的危险因素。高APACHE Ⅱ评分患者发生鲍曼不动杆菌血流感染的风险较低APACHE Ⅱ评分患者高(OR=1.163,P<0.05)[21],但也有研究[22]表明APACHE Ⅱ评分和CLABSI无相关性。
与其颈内静脉置管位点相比,股静脉置管患者CLABSI发病率增加6倍(OR=6.846,P<0.001),值得注意的是,本研究中大多CVC是通过颈内静脉插入,但其对CLABSI的危险较低。不同的文献研究对置管部位分析的结果有差异,有研究表明股静脉置管的风险较高,而锁骨下静脉置管的风险较低[23];而有研究[24]结果表明没有差异。主要原因是股静脉部位携带明显的腹股沟分泌物污染源,容易被排泄物污染[19]。一项对ICU患者CLABSI的干预研究[25]表明,干预后股静脉与多部位同时置管的比例减少,以及锁骨下静脉置管比例增加后,CLABSI发病率降低。对ICU患者CLABSI的Meta分析显示,股静脉置管发生感染的风险增加2.44倍[26],因此,很多临床实践指南建议应避免使用股静脉部位,但CVC的首选放置部位需要基于置管者的技能和专业知识,超声引导放置的可用性和专业知识,出血和其他并发症(气胸)的风险,以及放置的紧迫性最终来决定[23]。对于感染性和非感染性并发症,必须单独考虑不同置入部位的风险和益处,例如有颈静脉置管的患者如果同时进行气管造口术,可能有更高的感染风险。该院是当地最大三级综合医院,收治危重患者较多,由于在紧急和高风险的情况下,股静脉的置入途径往往具有更低的置入风险[27],因此本研究中感染组股静脉置管患者占比较高。
一项对西安地区的研究[28]结果表明,ICU患者静脉导管相关感染病原菌以革兰阳性菌为主,即凝固酶阴性葡萄球菌;随着时间变化,病原菌的流行病学发生变迁,革兰阴性菌占比越来越多[24, 29-30];一项对ICU患者CLABSI 5年病原学演变研究[31]结果表明,革兰阴性菌是CLABSI的主要致病菌。本研究CLABSI主要检出病原菌是革兰阴性的肺炎克雷伯菌,肺炎克雷伯菌是医院感染常见的条件致病菌,与一项前瞻性观察研究[32]结果一致,肺炎克雷伯菌占CLABSI的48%。也有研究[33]显示CLABSI最常见的病原菌是多重耐药鲍曼不动杆菌,占27.1%,可能是因为患者机体出现免疫力低下及大量使用广谱抗菌药物时,容易发生感染。
综上所述,本研究结果表明,引起CLABSI感染的独立危险因素有高APACHE Ⅱ评分、中心静脉置管时间长及股静脉置管。此外,CLABSI的流行病学趋向革兰阴性病原体。由于革兰阴性感染与高病死率有关,尤其是多重耐药菌,经验性治疗时应着重考虑。通过对CLABSI危险因素的研究和病原菌流行病学的监测,有助于尽早采取预防干预策略,同时也为CLABSI风险预测评分模型构建提供理论依据。
利益冲突:所有作者均声明不存在利益冲突。
-
图 1 倾向评分的分布图
Fig. 1 Distribution of propensity score
下载:
全尺寸图片
图 2 倾向评分分布直方图
注:AC为未匹配的直方图;BD为匹配后的直方图。
Fig. 2 Histogram of propensity score distribution
下载:
全尺寸图片
表 1 匹配前后两组患者基本临床资料
Table 1 Baseline characteristics of two groups of patients before and after matching
基本资料 匹配前 t/χ2 P SMD 匹配后 t/χ2 P SMD 感染组(n=44) 非感染组(n=4 366) 感染组(n=42) 对照组(n=168) 年龄(x±s,岁) 65.09±15.07 66.29±15.43 0.51 0.609 -0.079 65.38±15.34 67.45±15.39 0.78 0.436 -0.118 性别[例(%)] 1.66 0.198 0.186 0.61 0.433 0.012 男 24(54.5) 2 791(63.9) 24(57.1) 107(63.7) 女 20(45.5) 1 575(36.1) 18(42.9) 61(36.3) 糖尿病[例(%)] 15.09 < 0.001 0.509 0.70 0.401 -0.024 有 22(50.0) 1 073(24.6) 20(47.6) 68(40.5) 无 22(50.0) 3 293(75.4) 22(52.4) 100(59.5) 高血压[例(%)] 2.49 0.114 0.246 0.12 0.727 0.004 有 27(61.4) 2 157(49.4) 25(59.5) 95(56.5) 无 17(38.6) 2 209(50.6) 17(40.5) 73(43.5) 恶性肿瘤[例(%)] 0.03 0.868 -0.026 <0.01 1.000 0.087 有 6(13.6) 634(14.5) 5(11.9) 20(11.9) 无 38(86.4) 3 732(85.5) 37(88.1) 148(88.1) 心功能不全[例(%)] 15.77 <0.001 -0.603 - - <0.001 有 0(0) 1 155(26.5) 0(0) 0(0) 无 44(100) 3 211(73.5) 42(100) 168(100) 肾功能不全[例(%)] 8.91 0.003 0.454 0.18 0.676 -0.049 有 27(61.4) 1 714(39.3) 25(59.5) 94(56.0) 无 17(38.6) 2 652(60.7) 17(40.5) 74(44.0) 表 2 CLABSI病原体分布情况
Table 2 Distribution of pathogens causing CLABSI
病原体 菌株数 构成比(%) 革兰阳性菌 52 44.1 金黄色葡萄球菌 14 11.9 表皮葡萄球菌 10 8.5 人葡萄球菌 9 7.6 肠球菌 8 6.8 头状葡萄球菌 8 6.8 溶血葡萄球 3 2.5 革兰阴性菌 56 47.4 肺炎克雷伯菌 17 14.4 大肠埃希菌 13 11.0 鲍曼不动杆菌 10 8.5 铜绿假单胞菌 9 7.6 阴沟肠杆菌 7 5.9 真菌 10 8.5 白念珠菌 10 8.5 合计 118 100 表 3 匹配后两组患者CLABSI影响因素的单因素分析
Table 3 Univariate analysis on the influencing factors for CLABSI in two groups of patients after matching
因素 感染组(n=42) 对照组(n=168) t/χ2 P 因素 感染组(n=42) 对照组(n=168) t/χ2 P 中心静脉置管时间(x±s,d) 31.00±23.82 6.43±5.90 -14.24 <0.001 手术史[例(%)] 0.450 0.504 是 27(64.3) 117(69.6) APACHE Ⅱ评分(x±s,分) 27.55±8.37 20.84±5.85 -6.042 <0.001 否 15(35.7) 51(30.4) 使用呼吸机[例(%)] 2.470 0.115 是 11(26.2) 66(39.3) 置管部位[例(%)] 23.700 <0.001 否 31(73.8) 102(60.7) 颈内静脉 10(23.8) 89(53.0) 导尿管置管[例(%)] 0.214 0.643 锁骨下静脉 6(14.3) 40(23.8) 是 8(19.0) 27(16.1) 股静脉 26(61.9) 39(23.2) 否 34(81.0) 141(83.9) 使用抗菌药物[例(%)] 13.130 <0.001 白细胞计数[例(%)] 0.481 0.488 正常值组 17(40.5) 78(46.4) 是 42(100) 126(75.0) 异常值组 25(59.5) 90(53.6) 中性粒细胞计数[例(%)] 0.583 0.445 否 0(0) 42(25.0) 联合使用抗菌药物[例(%)] 10.683 0.001 正常值组 10(23.8) 50(29.8) 异常值组 32(76.2) 118(70.2) ≤2种 9(21.4) 83(49.4) C反应蛋白[例(%)] 5.241 0.022 正常值组 5(11.9) 49(29.2) ≥3种 33(78.6) 85(50.6) 异常值组 37(88.1) 119(70.8) 注:白细胞计数正常值为(3.5~9.5)×109/L;中性粒细胞计数正常值为(1.8~6.3)×109/L;C反应蛋白参考范围0~10 mg/L。 表 4 匹配后两组患者CLABSI多因素logistic回归分析
Table 4 Multivariate logistic regression analysis on CLABSI in two groups of patients after matching
因素 β Waldχ2 P OR 95%CI APACHE Ⅱ评分 0.196 12.478 <0.001 1.217 1.091~1.357 中心静脉置管时间 0.241 24.464 <0.001 1.273 1.157~1.400 颈内静脉置管(参照组) - 9.581 0.008 - - 锁骨下静脉置管 -0.409 0.197 0.657 0.664 0.109~4.036 股静脉置管 1.924 6.228 0.013 6.846 1.511~31.014 常量 -29.742 0 0.995 - - 注:-表示无数据。 -
[1] 孙宁鑫, 贾维慧, 宋艳梅, 等. ICU肠外营养患者中心静脉导管相关血流感染病原学分析及预测模型构建[J]. 护理学杂志, 2023, 38(20): 89-92. doi: 10.3870/j.issn.1001-4152.2023.20.089 Sun NX, Jia WH, Song YM, et al. Pathogens and prediction model for central line-associated bloodstream infections in intensive care unit patients receiving parenteral nutrition[J]. Journal of Nursing Science, 2023, 38(20): 89-92. doi: 10.3870/j.issn.1001-4152.2023.20.089 [2] 王敏, 杨昕, 周燕平, 等. ICU患者深静脉导管留置时间与导管相关血流感染的关系研究[J]. 检验医学与临床, 2019, 16(12): 1763-1766. doi: 10.3969/j.issn.1672-9455.2019.12.044 Wang M, Yang X, Zhou YP, et al. The relationship between duration of catheter insertion and central line-associated bloodstream infections in intensive care unit patients[J]. Laboratory Medicine and Clinic, 2019, 16(12): 1763-1766. doi: 10.3969/j.issn.1672-9455.2019.12.044 [3] Lissauer ME, Leekha S, Preas MA, et al. Risk factors for central line-associated bloodstream infections in the era of best practice[J]. J Trauma Acute Care Surg, 2012, 72(5): 1174-1180. doi: 10.1097/TA.0b013e31824d1085 [4] Ippolito P, Larson EL, Furuya EY, et al. Utility of electronic medical records to assess the relationship between parenteral nutrition and central line-associated bloodstream infections in adult hospitalized patients[J]. JPEN J Parenter Enteral Nutr, 2015, 39(8): 929-934. doi: 10.1177/0148607114536580 [5] Kim IJ, Shim DJ, Lee JH, et al. Impact of subcutaneous tunnels on peripherally inserted catheter placement: a multicenter retrospective study[J]. Eur Radiol, 2019, 29(5): 2716-2723. doi: 10.1007/s00330-018-5917-x [6] Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples[J]. Stat Med, 2009, 28(25): 3083-3107. doi: 10.1002/sim.3697 [7] 中华医学会重症医学分会. 血管内导管相关感染的预防与治疗指南(2007)[J]. 中国实用外科杂志, 2008, 28(6): 413-421. doi: 10.3321/j.issn:1005-2208.2008.06.001 Critical Care Medicine Branch of the Chinese Medical Association. Guidelines for prevention and treatment of vessel catheter associated infection(2007)[J]. Chinese Journal of Practical Surgery, 2008, 28(6): 413-421. doi: 10.3321/j.issn:1005-2208.2008.06.001 [8] Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects[J]. Biometrika, 1983, 70(1): 41-55. doi: 10.1093/biomet/70.1.41 [9] Ming K, Rosenbaum PR. Substantial gains in bias reduction from matching with a variable number of controls[J]. Biome-trics, 2000, 56(1): 118-124. [10] Al-Shukri RN, Al-Rawajfah OM, Al-Daken L, et al. ICU-acquired central line-associated bloodstream infection and its associated factors in Oman[J]. Am J Infect Control, 2022, 50(9): 1026-1031. doi: 10.1016/j.ajic.2021.12.024 [11] 吕倩, 赖晓全, 魏诗晴, 等. 应用精细化防控措施降低中心静脉导管相关血流感染发病率[J]. 中国感染控制杂志, 2022, 21(4): 363-367. doi: 10.12138/j.issn.1671-9638.20222145 Lv Q, Lai XQ, Wei SQ, et al. Application of precise prevention and control measures in reducing incidence of central venous catheter-related bloodstream infection[J]. Chinese Journal of Infection Control, 2022, 21(4): 363-367. doi: 10.12138/j.issn.1671-9638.20222145 [12] 王平. 中心静脉导管相关血流感染的危险因素及病原菌分析[D]. 太原: 山西医科大学, 2023. Wang P. Risk factors and pathogenic bacteria of central line-associated bloodstream infection[D]. Taiyuan: Shanxi Medical University, 2023. [13] 李怡, 王志翔, 李婧, 等. 2017—2019年某医院综合ICU医院感染目标监测分析[J]. 中华医院感染学杂志, 2021, 31(6): 929-932. Li Y, Wang ZX, Li J, et al. Targeted surveillance of nosocomial infection in ICU of a hospital from 2017 to 2019[J]. Chinese Journal of Nosocomiology, 2021, 31(6): 929-932. [14] Frasca D, Dahyot-Fizelier C, Mimoz O. Prevention of central venous catheter-related infection in the intensive care unit[J]. Crit Care, 2010, 14(2): 212. doi: 10.1186/cc8853 [15] Jansen SJ, Broer SDL, Hemels MAC, et al. Central-line-associated bloodstream infection burden among Dutch neonatal intensive care units[J]. J Hosp Infect, 2024, 144: 20-27. doi: 10.1016/j.jhin.2023.11.020 [16] Miliaraki M, Katzilakis N, Chranioti I, et al. Central line-associated bloodstream infection in childhood malignancy: single-center experience[J]. Pediatr Int, 2017, 59(7): 769-775. doi: 10.1111/ped.13289 [17] 杨婷, 李迎霞, 王晨钟, 等. 神经外科中心静脉导管相关血流感染病原学及死亡危险因素[J]. 中华医院感染学杂志, 2021, 31(1): 86-90. Yang T, Li YX, Wang CZ, et al. Etiological characteristics of central venous catheter-related bloodstream infection in neurosurgery department and risk factors for death[J]. Chinese Journal of Nosocomiology, 2021, 31(1): 86-90. [18] 李元叶, 袁欢欢, 王盟. 某医院重症监护病房住院患者导管相关血流感染病原菌特点及危险因素分析[J]. 中国消毒学杂志, 2020, 37(2): 108-110, 113. Li YY, Yuan HH, Wang M. Analysis of the characteristics and risk factors of CRBSI infection pathogens in ICU inpatients of a hospital[J]. Chinese Journal of Disinfection, 2020, 37(2): 108-110, 113. [19] Böll B, Schalk E, Buchheidt D, et al. Central venous catheter-related infections in hematology and oncology: 2020 updated guidelines on diagnosis, management, and prevention by the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO)[J]. Ann Hematol, 2021, 100(1): 239-259. doi: 10.1007/s00277-020-04286-x [20] Shahi S, Paneru H, Ojha R, et al. SOFA and APACHE Ⅱ scoring systems for predicting outcome of neurological patients admitted in a tertiary hospital intensive care unit[J]. Ann Med Surg (Lond), 2024, 86(4): 1895-1900. doi: 10.1097/MS9.0000000000001734 [21] 凌勇, 蔡依含, 叶龙, 等. 危重症监护室泛耐药鲍曼不动杆菌血流感染的危险因素及预后[J]. 临床与病理杂志, 2023, 43(8): 1539-1546. Ling Y, Cai YH, Ye L, et al. Risk factors and prognosis of extensively drug resistant Acinetobacter baumannii bloodstream infection in critical care unit[J]. Journal of Clinical and Pathological Research, 2023, 43(8): 1539-1546. [22] Walz JM, Ellison RT 3rd, Mack DA, et al. The bundle "plus": the effect of a multidisciplinary team approach to era-dicate central line-associated bloodstream infections[J]. Anesth Analg. 2015, 120(4): 868-876. doi: 10.1213/ANE.0b013e3182a8b01b [23] Pitiriga V, Kanellopoulos P, Bakalis I, et al. Central venous catheter-related bloodstream infection and colonization: the impact of insertion site and distribution of multidrug-resistant pathogens[J]. Antimicrob Resist Infect Control, 2020, 9(1): 189. doi: 10.1186/s13756-020-00851-1 [24] Moriyama K, Ando T, Kotani M, et al. Risk factors associa-ted with increased incidences of catheter-related bloodstream infection[J]. Medicine (Baltimore), 2022, 101(42): e31160. doi: 10.1097/MD.0000000000031160 [25] 范润平, 龚青霞, 巩文花, 等. ICU患者中心静脉导管血流感染危险因素的Meta分析[J]. 中国感染控制杂志, 2018, 17(4): 335-340. doi: 10.3969/j.issn.1671-9638.2018.04.012 Fan RP, Gong QX, Gong WH, et al. Meta-analysis on risk factors for central venous catheter-related blood-stream infection in intensive care unit patients[J]. Chinese Journal of Infection Control, 2018, 17(4): 335-340. doi: 10.3969/j.issn.1671-9638.2018.04.012 [26] Marschall J, Mermel LA, Fakih M, et al. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update[J]. Infect Control Hosp Epidemiol, 2014, 35(7): 753-771. doi: 10.1086/676533 [27] Health Protection Surveillance Center. Prevention of intravascular catheter-related infection in Ireland[EB/OL]. [2024-03-10]. https://www.hpsc.ie/a-z/microbiologyantimicrobialre-sistance/infectioncontrolandhai/intravascularivlines/publicatio-ns/File,4115,en.pdf. [28] 王慧萍, 王佩, 高艳玲, 等. 2020—2022年西安地区三甲医院重症医学科静脉导管相关血流感染病原菌特征及耐药性分析[J]. 华南预防医学, 2023, 49(12): 1551-1555. Wang HP, Wang P, Gao YL, et al. Pathogenic characteristics and drug resistance of venous catheter-related bloodstream infections in the intensive care department of class A tertiary hospitals in Xi'an, 2020-2022[J]. South China Journal of Preventive Medicine, 2023, 49(12): 1551-1555. [29] Lin KY, Cheng A, Chang YC, et al. Central line-associated bloodstream infections among critically-ill patients in the era of bundle care[J]. J Microbiol Immunol Infect, 2017, 50(3): 339-348. doi: 10.1016/j.jmii.2015.07.001 [30] 徐腾飞, 刘志武, 金凤玲. 2012—2015年医院血流感染病原菌分布及耐药性变迁[J]. 中国感染控制杂志, 2017, 16(10): 936-940. doi: 10.3969/j.issn.1671-9638.2017.10.009 Xu TF, Liu ZW, Jin FL. Changes in distribution and antimicrobial resistance of pathogens causing bloodstream infection in 2012-2015[J]. Chinese Journal of Infection Control, 2017, 16(10): 936-940. doi: 10.3969/j.issn.1671-9638.2017.10.009 [31] Lutufyo TE. ICU中心静脉相关血流感染五年的流行病学、危险因素和病原学演变[D]. 济南: 山东大学, 2022. Lutufyo TE. Five-year changes in epidemiology, risk factors and causative pathogens of central-line associated bloodstream infection in an intensive care unit population: a retrospective observational study[D]. Jinan: Shandong University, 2022. [32] Arunan B, Ahmed NH, Kapil A, et al. Central line-associated bloodstream infections: effect of patient and pathogen factors on outcome[J]. J Glob Infect Dis, 2023, 15(2): 59-65. doi: 10.4103/jgid.jgid_213_22 [33] Pitiriga V, Bakalis J, Kampos E, et al. Duration of central venous catheter placement and central line-associated bloodstream infections after the adoption of prevention bundles: a two-year retrospective study[J]. Antimicrob Resist Infect Control, 2022, 11(1): 96. doi: 10.1186/s13756-022-01131-w
